Classification of abdominal lymph nodes. Lymph nodes of the abdominal cavity. Normal Anatomy. Massaging the lungs and lymph nodes of the chest
A condition of the body in which the lymph nodes are enlarged abdominal cavity, namely in the mesentery, is called mesadenitis or mesenteric lymphadenitis. The nodes become larger in size due to the flow occurring inside them. Enlarged lymph nodes are not independent; it is rather a symptom of another pathology of various etiologies that affects the body.
Lymphadenopotia - mechanism of occurrence
Even a slight increase in lymph nodes in the human body is an alarming signal, since this indicates the occurrence of pathological process inside the body. kind of indicators. Pathogenic agents entering them cause a response, increased production lymphocytes. Because of this, the lymph node increases in size. As the pathology progresses, inflammation may develop in it. The lesion may involve one lymph node or several at once. Therefore, even hidden pathology in the body becomes obvious.
As stated earlier, swollen lymph nodes are not a disease, but chronic course inflammatory process may lead to the development of severe complications. Most often, with lymphadenitis, an acute course of the disease is observed. The affected node becomes larger, palpation causes pain, the skin over the surface of the lymph node is hyperemic, and the local temperature rises. These symptoms are quite indicative and require immediate medical attention.

As for mesenteric lymph nodes, their diagnosis is difficult. Since they are located in the peritoneal cavity, inflammation in them cannot be diagnosed without laboratory research and instrumental procedures.
Reasons for the development of pathology
It is impossible to accurately and unambiguously determine the causes of enlarged retroperitoneal and mesenteric lymph nodes. But this happens in to a greater extent because infections penetrate into the lymph nodes through the intestines or lymph.
The viruses, infections and bacteria listed above are pathogenic in nature and can affect any of the 500 lymph nodes located in the abdominal area.
Classification
Depending on how many lymph nodes are enlarged, the pathology is classified into three types:
- local;
- regional;
- generalized.
Local damage affects one lymph node. Regional enlargement of nodes affects several nodes located next to each other. As for the generalized development of pathology, this is the most severe case, since at least three groups of lymph nodes are involved, which are in different parts of the body.
About 70% of cases of enlarged lymph nodes occur in the local form of the pathology. Generalized inflammation in the nodes indicates serious problems in the functioning of the immune system.
Another type of classification subdivides lymphadenopathy according to the period of limitation:
- acute;
- chronic;
- recurrent.
Mesadenitis can take any of these three forms of the disease. But it is worth noting that in chronic form in the lymph nodes is already observed purulent inflammation, which spreads throughout the body.
Some experts use a classification of pathology according to the degree of hyperplasia, but this is a rather controversial division, since lymph nodes from different areas of the body vary in size even in normal condition.
Symptoms
Mesadenitis is a pathology, the existence of which people most often do not suspect. Abdominal lymph nodes are located inside the peritoneum, and their enlargement can only be diagnosed using ultrasound.

The mesentery is a fold of membrane that attaches the intestines to abdominal wall and holds it in place. Mesenteric lymphadenitis is inflammation of the lymph nodes in the mesentery
Diseases appear suddenly, and are more typical only when acute course. Patients suffer from pain in the abdominal area, in some cases it is impossible to indicate the exact location of the discomfort. If enlarged lymph nodes occur in the lower abdomen on the right, patients often confuse the pathology with appendicitis, since the pain and all the symptoms are very similar:
- Increased body temperature.
- Nausea and vomiting.
- Lack of appetite and stomach pain.
- Diarrhea or constipation.
- Tachycardia.
- Enlarged spleen and liver.
- Dry mouth, dehydration.
If symptoms are ignored for a long time, the patient may get unpleasant symptoms in the form of peritonitis, intestinal obstruction and others serious illnesses. This happens because the lymph nodes begin to fester without proper treatment.
The chronic form of the course is less noticeable to humans, clinical picture blurred and rarely causes concern. Pain syndrome practically absent, pain is felt only during physical activity.
Pathology often affects. According to statistics, girls get sick less often than boys. Age range from 6 to 13 years. The symptoms are no different from adult mesadenitis. When palpating the abdomen, you can find that it is tense, this is due to the formation of lymphoid follicles. It is necessary to consult a specialist to avoid complications and begin the necessary treatment on time.
Complications of mesenteric lymphadenitis
Mesadenitis requires treatment; if the pathology starts, it is incredibly dangerous for a person. If for a long time Do not contact a specialist; there is a risk of developing an abscess or peritonitis due to lymphatic suppuration.
Generalized lymphadenitis in extremely severe cases affects the entire lymphadenitis, as a result of which nodes throughout the body enlarge and become inflamed. These complications are especially common in patients suffering from tuberculosis; in other cases, this is a rather rare occurrence.
Establishing diagnosis
If you notice the above symptoms, you must immediately contact a specialist and undergo an examination. An accurate diagnosis requires a comprehensive laboratory instrumental examination of the patient. First of all, it is necessary to exclude inflammation of the appendix, since pain in the lower abdomen suggests this diagnosis.
The doctor initially collects an anamnesis of the disease. In order to identify the causative agent of the pathology, questions are asked about previous injuries, blood transfusions, transplantations, place of work, travel to Lately etc. During the examination, the specialist checks the condition of the mucous membranes and palpates the abdomen to determine the presence or absence of mesenteric follicles.
It is necessary to do a number of laboratory tests:
- General blood and urine analysis.
- Biochemical blood test.
- General stool analysis.
- Feces for occult blood.
- Serological tests.
- Wasserman test.
An accurate and unambiguous diagnosis can only be made after the results of an ultrasound or x-ray. Only after the cause of the disease has been established is it prescribed drug therapy. If you take measures only to eliminate symptoms, then relapses will occur after some time.
Treatment and prevention of pathology
Lymphadenitis is not a pathology that can be treated independently. Even when The lymph nodes increased without pain, you need to consult a specialist. Most effective therapy can only be prescribed by the attending physician, based on these studies.
The main part of the course of treatment is aimed at eliminating the disease, as a result of which the lymph nodes have enlarged. At positive effect inflammation in the nodes will decrease and they will decrease in size.
Most often used:
- Anti-inflammatory drugs.
- Antibacterial agents.
- Antiviral drugs.
- Immunomodulators, etc.
The prognosis for the treatment of mesadenitis is quite ambiguous, it all depends on the degree of pathology, the age of the patient and the cause that caused the enlargement of the lymph nodes. The main thing is to follow the doctor’s recommendations, which will help avoid the need for surgical intervention.
When the lymph nodes in the lower abdomen become enlarged, the patient feels sharp pain. In order to carry out differential diagnosis and find out the reasons for the development of pathology, you need to consult a doctor. The specialist will order a series of tests and prescribe medications. As a rule, for a complete recovery, it is enough to follow the doctor’s recommendations for 1-2 weeks, depending on the degree of progression of the underlying disease.
In the abdominal cavity there are also visceral (visceral) and parietal (parietal) lymph nodes.
Visceral lymph nodes (nodi lymphatici viscerales) are located near the unpaired visceral branches of the abdominal aorta and their branches (near the celiac trunk, hepatic, splenic and gastric arteries, superior and inferior mesenteric arteries and their branches). Celiac lymph nodes (nodi lymphatici coeliaci, 1-5 in total) are located near the celiac trunk on the paths of lymph flow from many visceral lymph nodes of the abdominal cavity. Approaches the celiac lymph nodes lymphatic vessels from the nodes of the stomach, pancreas and spleen, from the renal and hepatic lymph nodes. The efferent lymphatic vessels of the celiac nodes go to the lumbar lymph nodes and also flow into the initial part of the thoracic duct.
Gastric lymph nodes (nodi lymphatici gastrici) are located near the lesser and greater curvature of the stomach, along its arteries, and seem to surround the stomach. The left gastric lymph nodes (7-38) are located near the left gastric artery and its branches. These nodes are adjacent to the lesser curvature of the stomach and its walls (anterior and posterior). Lymphatic vessels flow into them, forming in the thickness of that part of the anterior and posterior walls of the stomach, which form its slight curvature. Lymph nodes located near the cardiac part (cardia) of the stomach and in the form of a chain covering the entrance part on all sides are called the lymphatic ring of the cardia (annulus lymphaticus cardiae, 1-11 in total), or “cardiac lymph nodes” (nodi lymphatici cardiaci - BNA ). The lymphatic vessels of the cardiac part of the stomach and its fundus, as well as from the abdominal part of the esophagus, are directed to these nodes.
The right gastric lymph nodes (1-3) are not permanent, located along the artery of the same name above the pylorus.
Pyloric lymph nodes (nodi lymphatici pilorici, 1-16 in total) are located above the pylorus, behind it and below it (on the head of the pancreas), next to the superior gastroduodenal artery. Lymphatic vessels flow into the pyloric nodes not only from the pylorus, but also from the head of the pancreas.
The right and left gastroepiploic nodes are located along the greater curvature of the stomach. They lie in the form of chains near the arteries and veins of the same name and receive lymphatic vessels that receive lymph from the walls of the stomach adjacent to the greater curvature, as well as from the greater omentum.
The right gastroepiploic lymph nodes (nodi lymphatici gastroomentalis dextri, total 1-49) are located in the gastrocolic ligament, at the right half of the greater curvature of the stomach, and are adjacent to the right gastroepiploic artery and vein. The left gastroepiploic lymph nodes (nodi lymphatici gastroomentalis sinistri, 1 - 17 in total) lie in the area of the left half of the greater curvature of the stomach, along the arteries and veins of the same name, between the layers of the gastrocolic ligament. At the upper edge of the pancreas (near the splenic artery and vein), on its posterior and anterior surfaces, there are pancreatic lymph nodes (nodi lymphatici pancreatici, 2-8 in total), which receive lymphatic vessels from the pancreas. The splenic lymph nodes are located in the hilum of the spleen, near the branching of the splenic artery and the formation of the splenic vein, in the thickness of the gastrosplenic ligament. Lymphatic vessels are directed to these nodes from the fundus of the stomach, the left gastroepiploic lymph nodes and from the spleen capsule.
Between the head of the pancreas and the wall duodenum at the place where the common bile duct flows into it, as well as near the branching point of the superior and inferior pancreaticoduodenal arteries, there are pancreaticoduodenal lymph nodes (nodi lymphatici pancreaticoduodenales), regional for the head of the pancreas and for the duodenum. One of the nodes of this group, usually large in size, is located behind the upper part of the duodenum and takes part in the formation of the anterior wall of the omental opening. Therefore, it received the corresponding name - the omental orifice node (nodus foraminalis). An increase in the size of this node can narrow the entrance to the omental bursa.
Hepatic lymph nodes (nodi lymphatici hepatici, 1-10 in total) are located in the thickness of the hepatoduodenal ligament along the common hepatic artery and portal vein. They are also located near the neck of the gallbladder - these are the gallbladder lymph nodes (nodi lymphatici cystici). There are only 1-2 of them, they receive lymphatic vessels from the liver and gall bladder. In rare cases (about 2%), the lymphatic vessels of the liver flow directly into the thoracic duct. The efferent lymphatic vessels of the hepatic and gall bladder lymph nodes go to the celiac and lumbar lymph nodes.
The largest group of visceral lymph nodes in the abdominal cavity is the mesenteric lymph nodes (nodi lymphatici mesenterici). There are from 66 to 404 of them, they are located in the mesentery small intestine near the superior mesenteric artery and vein, their branches and tributaries in the form of three subgroups. The first subgroup (peripheral) is located between the mesenteric edge of the small intestine and the vascular arches - arcades. These are peri-intestinal mesenteric nodes. The nodes of the second subgroup (middle) are adjacent to the trunks, branches and tributaries of the superior mesenteric artery and vein, and the nodes of the third - central subgroup are located near the superior mesenteric vessels along the length from the lower edge of the pancreas to the origin of the right colon artery. The lymph nodes of the central subgroup at the beginning of the superior mesenteric artery are quite closely adjacent to each other and in some cases form a kind of conglomerate.
From the jejunum and ileum, lymphatic vessels are directed mainly to the peripheral subgroup of mesenteric lymph nodes. Some lymphatic vessels bypass these nodes and follow to the nodes of the middle and even central subgroup. The efferent lymphatic vessels of the mesenteric lymph nodes (central subgroup) flow into the lumbar lymph nodes, and in some cases (about 25%) - directly into the thoracic duct, forming intestinal trunks (trunci intestinales). The lymphatic vessels of the terminal ileum flow not into the mesenteric, but into the ileocolic lymph nodes.
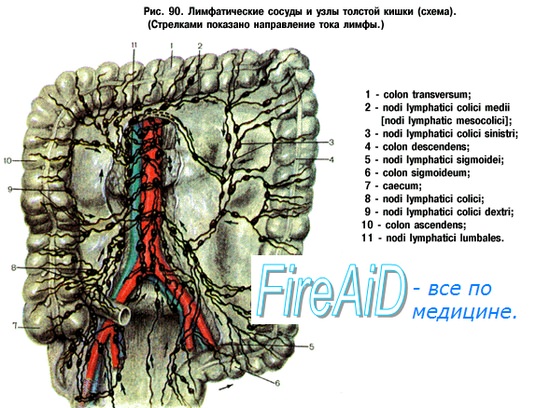
Regional lymph nodes colon are the nodes adjacent to the colon arteries and veins - branches and tributaries of the superior and inferior mesenteric arteries and veins. Lymphatic vessels carrying lymph from the cecum and appendix flow into numerous (3-15) relatively small cecal nodes (nodi lymphatici caecales). Among these nodes, the prececal and post-cecal lymph nodes (nodi lymphatici precaecales et retrocaecales), located respectively near the anterior and posterior walls of the cecum, are distinguished. Single lymphatic vessels of this organ, as well as the appendix, flow into the ileocolic lymph nodes (nodi fymphitici ileocolici, 1-7 in total), to which the lymphatic vessels of the final section of the ileum are also directed. The lymphatic vessels of the ascending colon flow into the right colon lymph nodes (nodi lymphatici colici dextri, 7-55 in total), located near the right colon arteries and veins, their branches and tributaries. From the descending colon and sigmoid colon lymphatic vessels are directed to the left colon lymph nodes (nodi lymphatici colici sinistri, total 8-65) and to the sigmoid lymph nodes (nodi lymphatici sigmoidei, total 5-50), which are located near the arteries and veins of the same name, their branches and tributaries. Lymphatic vessels from the upper part of the rectum also approach the sigmoid lymph nodes. The efferent lymphatic vessels of the sigmoid and left colic lymph nodes follow to the lower mesenteric nodes (nodi lymphatici mesenterici inferiores), and the efferent vessels of the latter flow into the lumbar lymph nodes located near the abdominal aorta and the inferior pudendal vein (pariental nodes of the abdominal cavity).
On the paths of the lymphatic vessels from the colon to its regional lymph nodes (colic), there are not very large paracolic nodes (nodi lymphatici paracolici). They are located directly next to the medial (lower - for the transverse colon) wall of the intestine or near it.
The efferent lymphatic vessels of the ileocolic, mesenteric-colic, right and left colic lymph nodes are directed to the parietal lumbar lymph nodes, as well as to the central subgroup of the superior mesenteric lymph nodes, located at the beginning of the superior mesenteric artery and near the vein of the same name.
Parietal lymph nodes (nodi lymphatici parietales) of the abdominal cavity are located on the anterior abdominal wall (lower epigastric) and on the posterior abdominal wall (lumbar). The lower epigastric lymph nodes (nodi lymphatici epigastrici inferiores, 3-4 in total) are paired, lie in the thickness of the anterior abdominal wall along the course of the same blood vessels. These nodes collect lymph from the adjacent parts of the rectus, transverse and oblique abdominal muscles, the peritoneum lining the anterior abdominal wall, and from the subperitoneal tissue. The efferent lymphatic vessels of these nodes are directed along the lower hypogastric blood vessels down to the external iliac, and up along the upper epigastric vessels, and then along the internal thoracic blood vessels to the periosternal lymph nodes.
Numerous lumbar lymph nodes (nodi lymphatici lumbales, 11-41 in total) are located throughout the posterior abdominal wall (retroperitoneal) near the aorta and posterior vena cava. Due to the position of these nodes in relation to large vessels, they are divided into left, right and intermediate lumbar lymph nodes. The left lumbar lymph nodes (left lateroaortic) are adjacent in the form of a chain to the abdominal aorta on the left, front and back. In the group of these nodes, in turn, the following are distinguished: lateral aortic (nodi lymphatici aortici laterales, total 1-17), preaortic (nodi lymphatici preaortici, total 1-14) and postaortic (nodi lymphatici postaortici, total 1-15).
The right lumbar lymph nodes are located near the anterior, posterior and right surfaces of the inferior vena cava along the entire length from the place of its formation from the common iliac veins to the diaphragm. These lymph nodes are divided into precaval (nodi lymphatici precavales, total 1-7), postcaval (nodi lymphatici postcavales, total 1-12) and lateral caval (nodi lymphatici cavales laterales, total 1-4). In the groove between the abdominal part of the aorta and the inferior vena cava there is a chain of intermediate lumbar (interaortocaval) lymph nodes (nodi lymphatici lumbales intermedin 1-9 in total).
The listed lumbar lymph nodes, together with the lymphatic vessels connecting them, form a dense lymphatic plexus near the abdominal aorta and the inferior vena cava. Lymph from the lower extremities, walls and pelvic organs passes through the lumbar lymph nodes. The efferent lymphatic vessels of the lymph nodes located near the lymph nodes also flow into these nodes. internal organs abdominal cavity (gastric, mesenteric, colon, etc.).
The efferent lymphatic vessels of the lumbar lymph nodes form the right and left lumbar trunks, giving rise to the thoracic duct, or flow into the initial part of the duct independently.
On the posterior abdominal wall, near the inferior phrenic artery, paired non-permanent inferior phrenic lymph nodes of the same name (nodi lymphatici phrenici inferiores, 1-3 in total) are distinguished. They are also parietal parietal lymph nodes of the abdominal cavity. The lymphatic vessels of the diaphragm and the posterior parts of the right and left lobes of the liver flow into these nodes. The efferent lymphatic vessels of the lower phrenic nodes go to the celiac, postcaval and intermediate lumbar lymph nodes.
],Lymph nodes of the abdominal cavitydivided into visceral, located along the trunks and branches of the celiac trunk, superior and inferior mesenteric arteries, and parietal, or lumbar, lying around the aorta and inferior vena cava. The lumbar nodes (nodi lymphatici lumbales), in turn, are divided into left and right lateroaortic and pre- and retroaortic.
The left lateroaortic nodes (from 2 to 14 in number) are located in one or two rows along the left surface of the aorta, from its bifurcation to aortic orifice diaphragm. They are a continuation of the external chain of the left superior iliac nodes and from them the truncus lumbalis sinister arises in the form of one or several trunks. If there are several left lumbar trunks, then the one that connects to the right lumbar trunk is the main one, while the others are additional. The latter most often flow into the thoracic duct.
The right lateroaortic nodes consist of latero-, pre- and retrocaval and interaortocaval nodes. The chain of laterocaval nodes (1-8) starts from the node lying in the angle between the common iliac artery and the inferior vena cava, and ends above the right renal pedicle on the crus dextrum of the diaphragm. The efferent vessels of the nodes go to the retrocaval nodes, into the right transdiaphragmatic path and take part in the formation of the main roots of the thoracic duct. Efferent vessels from the lower precaval nodes (1-7 in number) above the beginning of the inferior mesenteric artery enter either the interaortocaval, preaortic, or retrocaval nodes. The upper non-permanent 1-2 precaval nodes lie on the anterior surface of the vein between the confluence of the renal vein and the beginning of the inferior mesenteric artery.
Retrocaval nodes (1-9) are located behind the inferior vena cava. Of these, we can distinguish the largest and most permanent node (the main one), which lies below the level of the confluence of the left renal vein into the inferior vena cava. The efferent vessels of the lower retrocaval nodes most often flow into the main retrocaval node, the efferent vessels of which are the main sources of the single or double right lumbar trunk, and less often into the right lumbar lymphatic trunk. Interaortocaval lymph nodes (1-5) are located between the aorta and the inferior vena cava along the level from the origin of the inferior mesenteric artery to the celiac trunk. Immediately below the left renal vein lies the main node of this chain, into which the lymphatic vessels of the testicle (or ovary), the efferent vessels of the central mesenteric and posterior pancreaticoduodenal nodes, kidneys, and liver flow. The outlet vessels of the node most often flow into the truncus lumbalis dexter.
Preaortic nodes are located on the anterior surface of the aorta at different levels: immediately above the aortic bifurcation (from 1 to 4 nodes), around the beginning of the inferior mesenteric artery (from 1 to 7 nodes). In the area from the inferior mesenteric artery to the lower edge of the left renal vein there are from 1 to 5 nodes. Large vessels flow into them from the central mesenteric nodes, posterior pancreatoduodenal and retropancreatic nodes. Above and behind the pancreas, at its lower edge, as well as above the left renal vein, lie the preaortic retropancreatic nodes (1-4), into which lymph flows from the celiac, hepatic, splenic and mesenteric nodes. At the base of the truncus coeliacus there are 1-2 large node, which are part of the nodi lymphatici coeliaci, lying along the branches of the celiac trunk. Their drainage vessels go to the upper left lateroaortic, to the retro- and laterocaval nodes and to the preaortic retropancreatic nodes. Retro-aortic nodes (1-4) are located behind the aorta along its entire length, connecting the left lateroaortic nodes with the retrocaval or interoaortocaval nodes.
The right lumbar lymphatic trunk (truncus lumbalis dexter) arises from the discharge vessels of the right lateroaortic and even preaortic nodes, which connect in various combinations and form a single or multiple (up to three) trunk. Accessory trunks flow into the thoracic duct. The right lumbar trunk is often located between abdominal aorta and the inferior vena cava, less often behind the vein or aorta. The fusion of the lumbar trunks forms the thoracic duct.
▪ FIGURE 92-1 Illustration of the upper gastrointestinal tract depicting the lymph nodes of stomach, liver, gallbladder, pancreas, and spleen: 1, celiac; 2, gastric (right and left); 3, gastroepiploic (right and left); 4, pyloric; 5, superior pancreatic; 6, inferior pancreatic; 7, perisplenic; 8, superior pancreaticoduodenal; 9, inferior pancreaticoduodenal; 10, cystic.
▪ FIGURE 92-2 Illustration of the retroperitoneum depicting the retroperitoneal lymph nodes: 1, celiac; 2, superior mesenteric; 3, inferior mesenteric; 4, para-aortic; 5, postaortic; 6, paracaval; 7, precaval; 8, postcaval; 9, aortocaval.
▪ FIGURE 92-3 Illustration of the colon with its arterial anatomy depicting the lymph nodal system of the colon: 1, superior mesenteric; 2, inferior mesenteric; 3, ileocolic; 4, right colic; 5, middle colic; 6, left colic; 7, sigmoid; 8, superior rectal; 9, paracolic; 10, prececal; 11, retrocecal; 12, appendicular.
.jpg)
▪ FIGURE 92-4 Illustration of the frontal view of the pelvis showing the pelvic lymph nodes: 1, median common iliacus; 2, intermediate common ilic; 3, lateral common iliacus; 4, subaortic common iliacus; 5, common iliac nodes of promontory; 6, medial external ilia; 7, intermediate external ilic; 8, lateral external ilic; 9, femoral (medial); 10, femoral (intermediate); 11, femoral (lateral); 12, obturator.
▪ FIGURE 92-5 Illustration of the lateral view of the pelvis showing the pelvic lymph nodes: 1, superior gluteal; 2, nodes along internal ilic branches; 3, sacral; 4, external iliac; 5, prevesical; 6, paravaginal; 7, lateral vesicular; 8, parauterine; 9, perirectal.

▪ FIGURE 92-6 Representative axial contrast-enhanced MDCT images of the abdomen and pelvis at various levels demonstrating the normal location of the abdominal lymph nodes. A: 1, Retrocrural. B: 2A, Perigastric nodes. C: 2, Gastrohepatic ligament. D: 3, Portohepatic; this image also shows an accessory spleen ( black arrow) at the splenic hilum that can mimic an enlarged lymph node. However, the accessory spleen shows attenuation and enhancement characteristics similar to native spleen. E: 4, Pancreaticoduodenal. F: 5, Perisplenic. G: 6, Mesenteric. H: 7, Celiac. I: 8, Superior mesenteric; 4, pancreaticoduodenal. J: 9, aortocaval. K: 10, Para-aortic; 11, retrocaval; 12, paracaval. L: 13, External iliac. M: 14, Internal ilic. N: 15, Obturator. O: 16, Common ilic. P: 17, Superficial inguinal; 18, deep inguinal.
4. Thoracic duct (ductus thoracicus). Topography, structure of the thoracic duct.
5. Right lymphatic duct (ductus lymphaticus dexter). Topography, structure of the right lymphatic duct.
6. Lymph nodes and vessels of the lower limb (leg). Topography, structure, location of lymph nodes and vessels of the leg.
7. Lymph nodes and vessels of the pelvis. Topography, structure, location of the lymph nodes and vessels of the pelvis.
8. Lymph nodes and vessels of the abdominal cavity (stomach). Topography, structure, location of lymph nodes and vessels of the abdominal cavity (stomach).
9. Lymph nodes and vessels of the chest. Topography, structure, location of the lymph nodes and vessels of the chest.
10. Lymph nodes and vessels of the upper limb (arm). Topography, structure, location of lymph nodes and vessels of the upper limb (arm).
11. Lymph nodes and vessels of the head. Topography, structure, location of the lymph nodes and vessels of the head.
12. Lymph nodes and vessels of the neck. Topography, structure, location of lymph nodes and vessels of the neck.
Lymph nodes and vessels of the abdominal cavity (stomach). Topography, structure, location of lymph nodes and vessels of the abdominal cavity (stomach).
Lymphatic vessels of the upper half of the abdominal wall directed upward and laterally towards nodi lymphatici axillares; the vessels of the lower half of the abdominal wall, on the contrary, descend to nodi lymphatici inguinales.
In the abdominal cavity there are: 1) parietal nodes, lying around the aorta and inferior vena cava, and 2) visceral, which are distributed along the trunks and branches of the celiac trunk, superior and inferior mesenteric arteries. The number of parietal nodes reaches 30 - 50. The general name of these “lumbar” nodes, nodi lymphatici lumbales.
Visceral nodes of the abdominal cavity fall into two large groups: 1) along the branches of the celiac trunk, 2) along the branches of the mesenteric arteries, nodi lymphatici mesenterici superkkes et inferiores.
Lymph nodes of the first group are named in relation to arteries and organs: nodi lymphatici coeliaci, gastrici sinistri et dextri, hepatici, pancreaticoduodenales, pylorici.
The second group of visceral nodes, located along the mesenteric arteries, is distinguished by its large number (about 300). It is embedded in the thickness of the mesentery of the small and large intestine and was described together with their lymphatic vessels. The lymphatic vessels of the abdominal organs flowing into the listed lymph nodes are described when describing the anatomy of each organ (see “Splanchnology”).
The small intestine has a special system of lymphatic vessels- system of milk vessels. The intestine contains a plexus of lymphatic vessels in all layers that make up its wall: mucosa, submucosa, muscular and serous.
At the same time, they distinguish two groups of lymphatic vessels:
1. Lymphatic vessels of the serous membrane.
2. Chyle, or milky vessels (chylus - milky juice) have their roots in central lymphatic vessels that begin blindly under the epithelium, at the top of the villus. They lie in the mucous membrane and submucosa of the intestine, then continuing into the mesentery, and transport absorbed fat, which gives the lymph the appearance of a milky emulsion (chyle), hence the name of these vessels (Fig. 258). Rest nutrients absorbed by the venous system and carried to the liver through the portal vein.
Efferent lymphatic vessels of the duodenum go to the pancreaticoduodenal lymph nodes. The draining lymphatic vessels of the jejunum and ileum go deep into the mesentery to the mesenteric nodes.
In the mesentery of the small intestine, three groups of lymphatic vessels should be distinguished:
1) left group - from the initial segment of the colon (40 - 70 cm), 2) middle group- from the rest of the jejunum and 3) the right group - from the ileum.Passing through the mesentery, lacteal vessels are interrupted by mesenteric lymph nodes, arranged in four rows. The nodes of the first row are located along the mesenteric edge of the intestine, the nodes of the second - slightly away from the edge, the nodes of the third - near the root of the mesentery, and the nodes of the fourth - at the root of the mesentery. From the mesenteric nodes, lymph flows to the lumbar nodes, and from there to truncus lumbalis sinister and further into the thoracic duct. Sometimes part of the efferent vessels of the mesenteric and other visceral nodes of the abdominal cavity is collected in short trunks called trunci intestinales, which flow either directly into the beginning of the thoracic duct, or into the left (rarely into the right) lumbar trunk.
From the colon, lymphatic drainage occurs in nodi lymphatici ileocolici, colici dextri, colici medii, mesenterici inferiores, colici sinistri, located along the vessels of the same name.




